




If your thyroid panel comes back showing a high TSH, you're probably wondering what that actually means and what you should do next. The short answer is that an elevated TSH usually points to your thyroid not producing enough thyroid hormone — but the next step isn't always to start thyroid medication. The bigger picture matters. This guide walks through how the TSH feedback loop works, what a high TSH is really telling you, and the questions that determine whether treatment is appropriate.
How TSH And Thyroid Hormone Talk To Each Other
TSH stands for thyroid-stimulating hormone. It's released by the pituitary gland in your brain, and its job is to signal the thyroid gland in your neck to produce thyroid hormones — primarily T4 (thyroxin), which then converts to T3 (the active form) in tissues throughout the body.
The simplest way to think about this system is like a thermostat. Your brain has a "set point" for the amount of T4 it expects to see floating around in the blood. When T4 drops below that set point, the brain (specifically the pituitary) increases TSH output, which tells the thyroid: "more, please." When T4 rises back to or above the set point, the brain lowers TSH and the thyroid backs off. It's a continuous feedback loop.
So when your TSH comes back high, what your brain is saying is: "I'm not seeing enough T4 — turn up production." That's a signal from the brain, not from the thyroid itself.
What A High TSH Actually Means
If TSH is elevated, there are two main scenarios driving it:
Scenario one (most common): the thyroid isn't producing enough thyroid hormone. The pituitary is doing its job, sending a strong signal, but the thyroid gland isn't responding adequately. This is the picture of primary hypothyroidism — and it's by far the most common reason for a high TSH. Hashimoto's thyroiditis (autoimmune destruction of thyroid tissue) is the most frequent underlying cause in adults. Iodine deficiency, post-surgical changes, post-radiation effects, and certain medications can also drive it.
Scenario two (less common): the brain isn't getting the feedback signal correctly. Even though plenty of T4 may be circulating, the pituitary isn't reading it accurately. This is rarer and tends to involve more complex pituitary or hypothalamic issues.
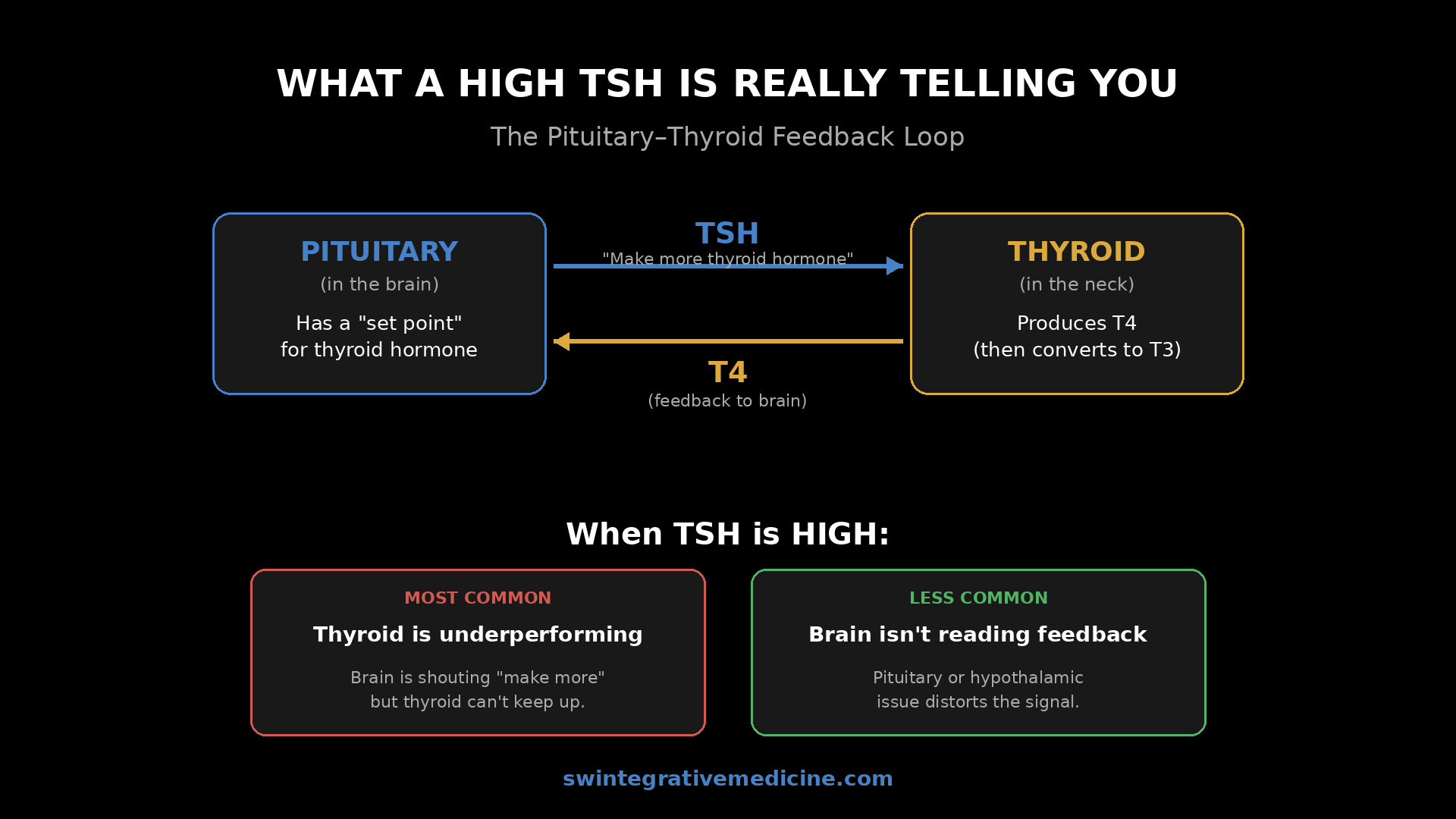
For most people, an elevated TSH means the thyroid gland is underperforming and the brain is shouting at it to do more.
What You Might Feel With An Elevated TSH
A high TSH (and the low thyroid hormone driving it) can produce a wide range of symptoms because thyroid hormone affects nearly every tissue in the body. The classic ones:
Fatigue. Cold intolerance. Weight gain that's hard to shift. Constipation. Dry skin. Hair thinning. Brain fog and slowed thinking. Low mood. Slower heart rate. Heavier or more irregular periods.
None of these symptoms are exclusive to thyroid problems, which is why the lab test matters — and why a single elevated TSH alone isn't always the whole story.
The Question Of Whether To Treat
If your TSH is high and your thyroid hormone is clearly low, the next step is usually thyroid hormone support. That can be levothyroxine (T4), a combined T4/T3 medication, or natural desiccated thyroid — depending on the case. The goal is to give the body the thyroid hormone it isn't producing on its own.
But not every elevated TSH gets treated, and the decision depends on the overall picture. Some questions I work through with patients:
Do you actually have low thyroid hormone symptoms? The clinical picture matters. A modestly elevated TSH with no symptoms is a different situation from one with classic hypothyroid symptoms.
Do you actually have low thyroid hormone in the blood? A high TSH with normal free T4 and free T3 is called subclinical hypothyroidism. It's a real category, but the threshold for treating it is more nuanced.
Is the elevation persistent? Has it shown up on multiple thyroid tests over time, or is it from one snapshot? TSH can be transiently elevated due to acute illness, recent stress, or even certain medications. Repeating the test 6 to 8 weeks later is often the right move before starting therapy.
How high is "high" — and where in the range are your free hormones? A TSH at 5.5 with free T4 in the lower half of the range is a different story from a TSH of 12 with low-normal free T4 and clear hypothyroid symptoms.
Are antibodies present? Thyroid peroxidase (TPO) antibodies and thyroglobulin antibodies tell you whether autoimmune thyroiditis is the underlying mechanism. That changes both the treatment plan and the long-term outlook.
What "Normal" Means For TSH
The standard reference range for TSH varies by lab but typically runs from about 0.4 to 4.5 mIU/L. Functionally, I tend to look at narrower targets — most patients feel best with TSH in the 1.0 to 2.5 range, and many feel notably better when their TSH is closer to 1.
A TSH of 4.0 might be technically "in range" but is on the higher end and worth watching, especially if free T4 is lower in its range or if symptoms are present. The reference range alone can't tell you whether your thyroid is functioning optimally for you.
What Tests To Run Beyond TSH
If you have an elevated TSH, the workup I want to see is broader than just one number:
Free T4. The amount of unbound, available thyroid hormone in circulation.
Free T3. The active form. Some people convert T4 to T3 poorly, and they can have normal-looking T4 with low T3 and full hypothyroid symptoms.
Reverse T3. When the body is under chronic stress or has certain illnesses, it can shunt T4 toward reverse T3 instead of active T3 — making thyroid hormone effectively unavailable to tissues even when total levels look fine.
TPO and thyroglobulin antibodies. To rule in or out Hashimoto's.
Repeat after 6 to 8 weeks. Confirm the pattern is stable before making a treatment decision.
Conclusion
A high TSH is your brain telling your thyroid to work harder — almost always because the thyroid isn't producing enough thyroid hormone. The right response depends on the full picture: symptoms, the actual levels of free T4 and free T3, antibody status, and whether the elevation persists over time.
Don't accept a single elevated TSH as a diagnosis without the rest of the workup, and don't ignore a borderline-high TSH if you have classic symptoms. Both errors are common, and both lead to people feeling worse than they need to.
If you've got an elevated TSH and you want help interpreting the rest of the picture — symptoms, antibodies, free hormones, conversion — work with me directly to build a treatment plan that fits your situation, not just the lab number.
Topics: TSH, Thyroid, Hypothyroidism, Hashimotos, Thyroid Hormone, Free T4, Free T3, Endocrinology










